A 70-year-old man presented to the AED with acute chest discomfort and SOB. His BP was 110/50 mmHg and SaO2 was 96% on 1L oxygen.
Which of the following is the most appropriate next step in management?
Choose the correct answer.
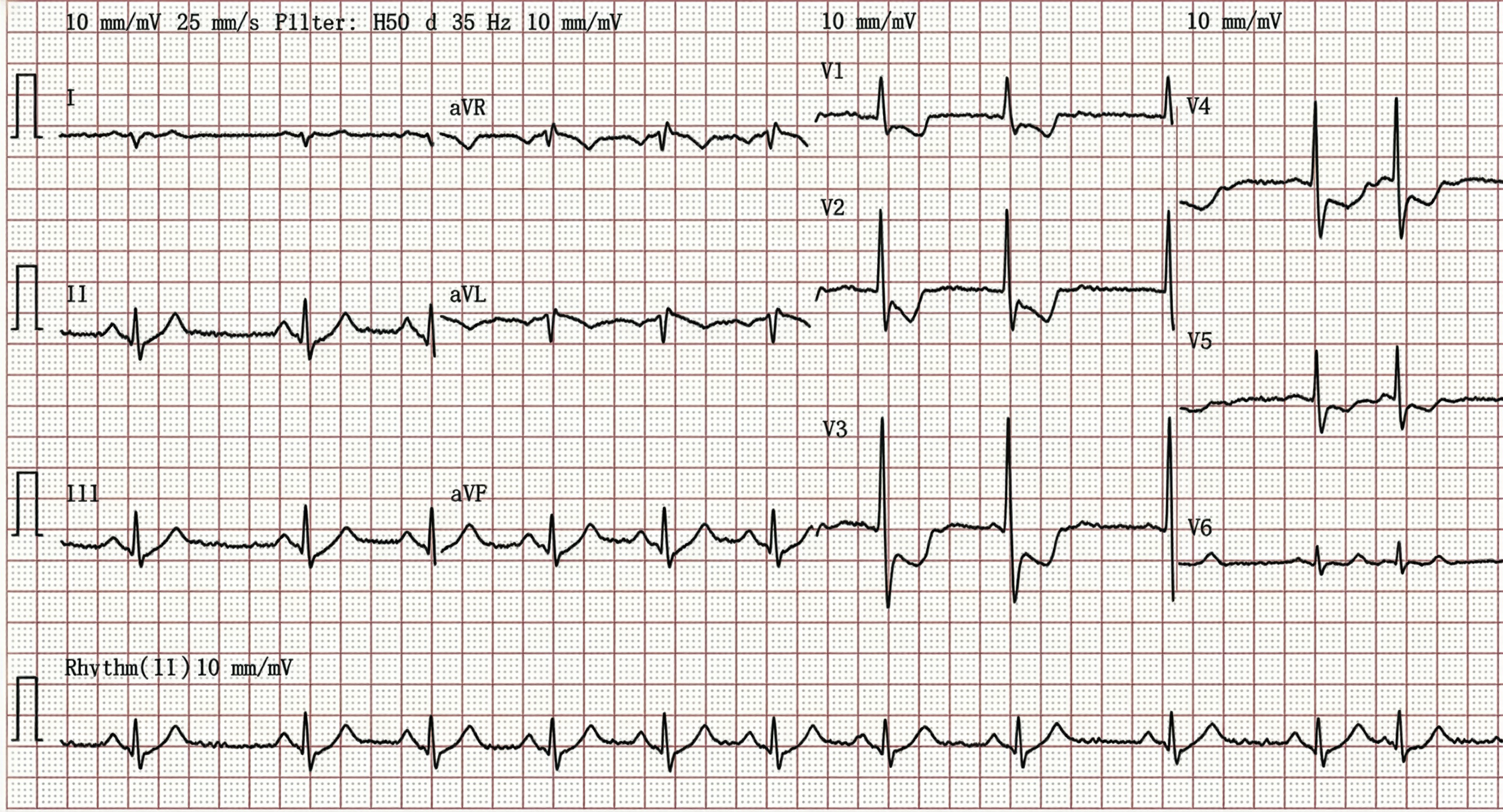
The ECG demonstrates ST-segment depression in leads V1–V3 with prominent R waves, a pattern highly suggestive of posterior STEMI. In such cases, the diagnosis could be further supported by evaluating the extended posterior leads V7–V9, which may reveal diagnostic ST elevation in some patients. Echocardiography provides crucial diagnostic verification when ECG findings remain equivocal. The most definitive finding is localized wall motion abnormality specifically involving the posterior segment of the left ventricle.
ST-T wave abnormalities associated with digoxin toxicity are usually diffuse and present across multiple leads, distinguishing them from the localized ischemic changes of a posterior infarction.
The most common ECG finding in pulmonary embolism (PE) is sinus tachycardia. In some patients, ECG findings may reflect acute right ventricular overload, manifesting as a new right bundle branch block (RBBB) or T-wave inversions in leads V1–V3, though significant ST-segment depression is less frequent. While the classic 'S1Q3T3' pattern (characterized by a deep S-wave in lead I, alongside a Q-wave and inverted T-wave in lead III) is suggestive of acute right heart strain, it is an infrequent finding with low sensitivity in clinical practice.
The presence of clearly identifiable P waves despite fluctuations in the atrial and ventricular rates is compatible with sinus arrhythmia rather than Atrial fibrillation.
