An 80-year-old woman presented to the AED with progressive SOB and chest discomfort for 3 days. She also experienced an episode of near-syncope. Her SaO2 was 94% on 4L O2 and her chest X-ray showed clear lung fields.
Which of the following statement(s) is/are correct?
Choose the correct answer.
Acute coronary syndrome must be considered in the presence of chest pain or its anginal equivalent combined with new electrocardiographic changes. However, a clear chest X-ray is entirely disproportionate to the severe degree of the patient's respiratory failure.
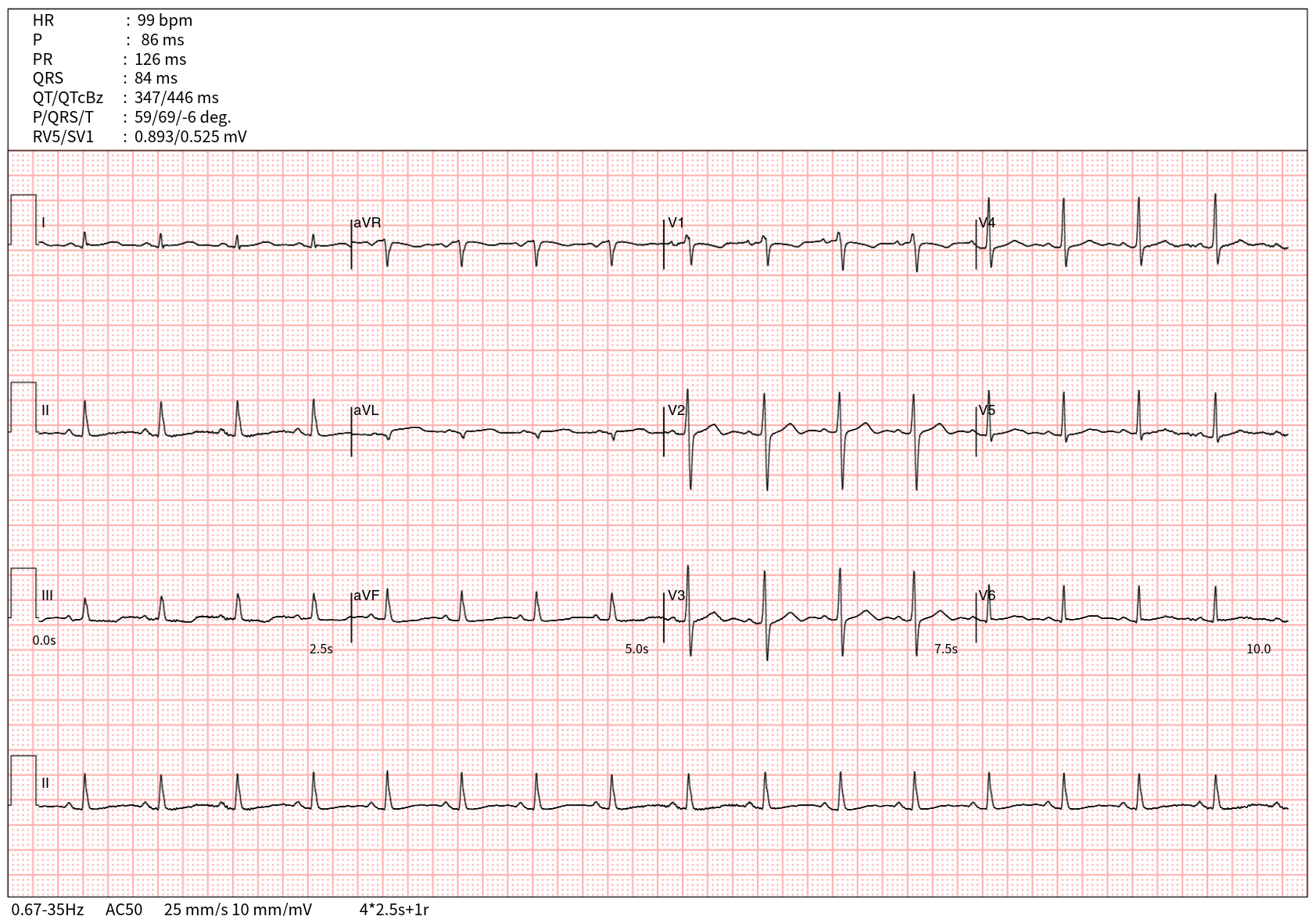
When the right ventricle (RV) is subjected to acute pressure or volume overload (increased wall stress), the normal ventricular activation sequence alters.
The resulting electrophysiological modifications include:
1. Prolonged Action Potential Duration: The stressed, ischemic, or mechanically stretched RV myocardium experiences a prolongation of its action potential.
2. Altered Transmural Dispersion: The standard direction of repolarization reverses, moving paradoxically from the endocardium to the epicardium.
3. Electrical Vector Shift: Because the repolarization wave propagates away from the exploring precordial leads (i.e., moving from the interventricular septum toward the RV free wall), the ECG records this vector shift as a negative (inverted) T wave.
Given that the RV is typically anteriorly and relatively inferiorly oriented—particularly within the geometric thoracic variations seen in elderly patients—these dynamic T-wave changes manifest most prominently in leads V1-3 and the inferior leads (II, III, aVF).
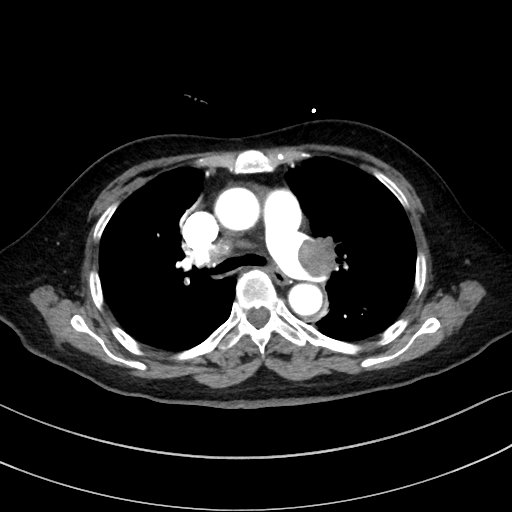
An urgent CT pulmonary angiogram was performed and confirmed the diagnosis of Acute pulmonary embolism.
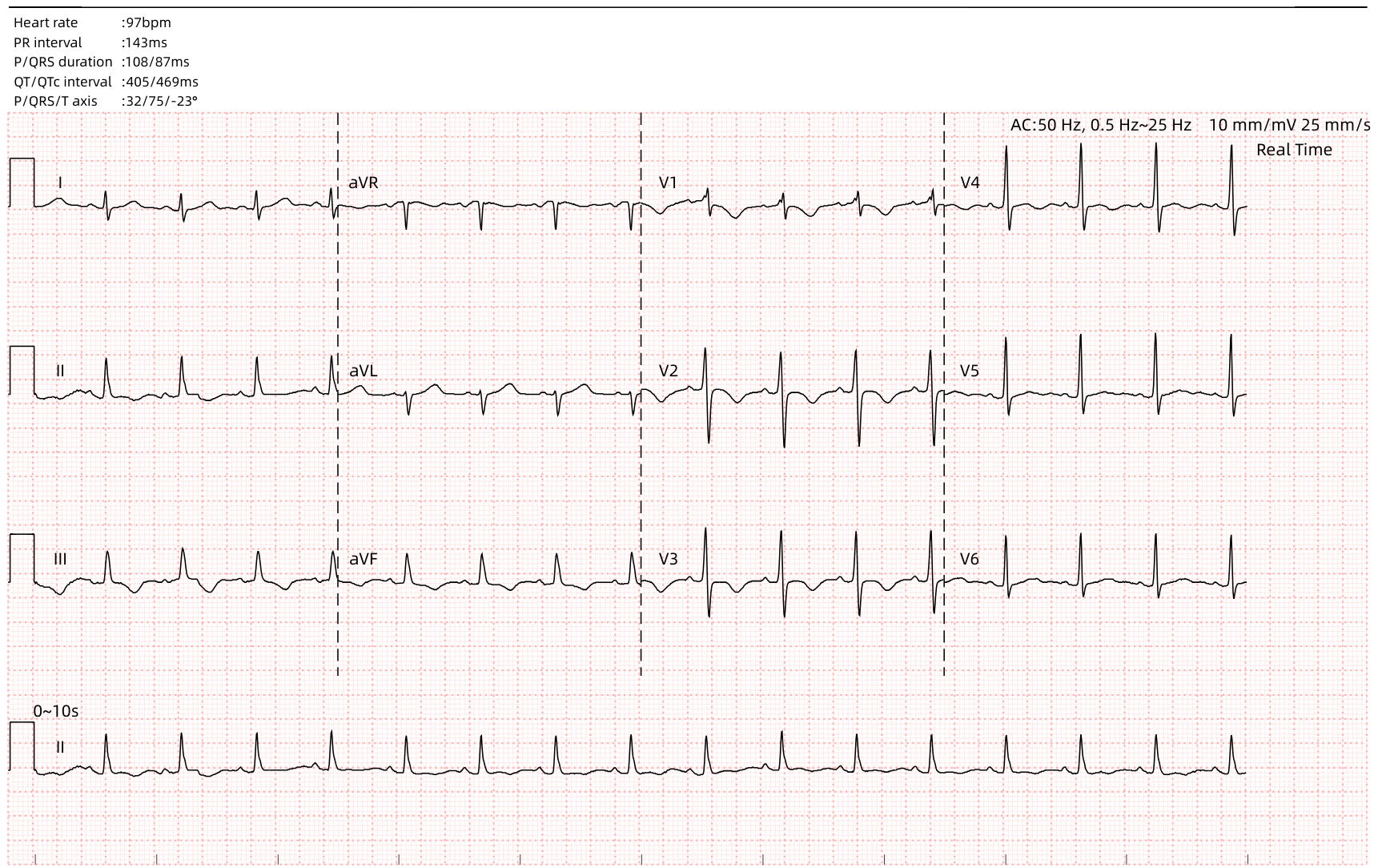
Her ECG was nearly normalised after mechanical thrombectomy.