A 40-year-old female presented to the AED with palpitations and dizziness. She recently had a viral illness and had taken unknown over-the-counter medications. Her blood pressure was 110/50 mmHg.
Whichof the following stagement is correct?
Choose the correct answer.
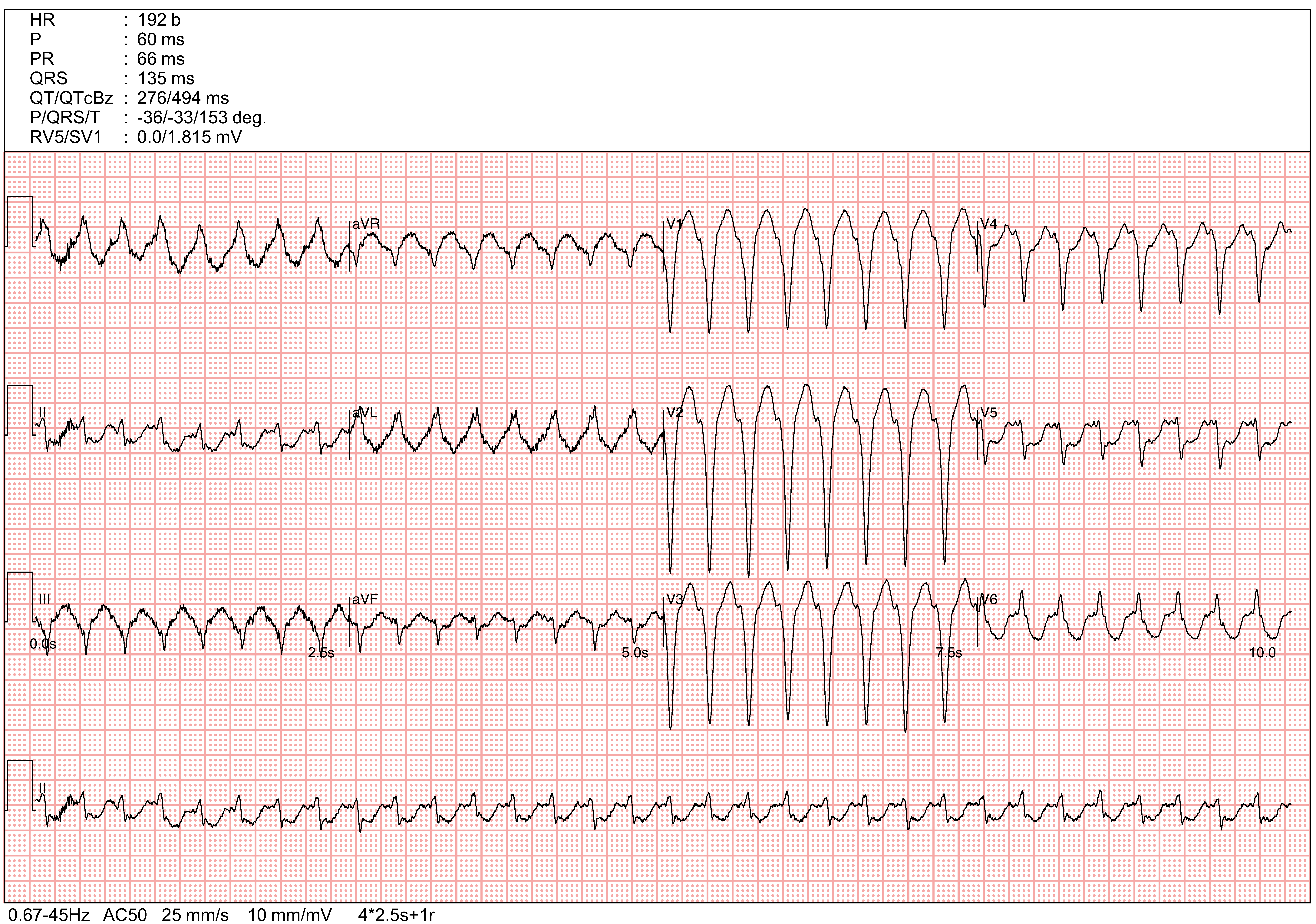
The ECG shows a regular wide complex tachycardia (WCT) with left bundle branch block (LBBB) morphology and superior axis (negative QRS polarity in lead III/aVF) at a rate of 192 bpm. The QRS duration was <100ms. The lead II/III and aVR/aVL leads shows polarity discordance (positive polarity in lead II and negative polarity in lead III; positive polarity in aVL and negative polarity in aVR). The precordial QRS transition was in V6.
The aVR shows rS morphology with the initial 40ms QRS amplitude < the terminal 40ms QRS amplitude (Vi/Vt <1). The QRS morphology does not strictly fulfill typical LBBB morphology features. Typical LBBB morphology feature is defined as (1) : QRS >=120ms with QS or rS morphology in V1, monophasic R wave with no Q wave in V6 and lead I, mid QRS notching or slurring in V5, V6, lead I and aVL). There were suspected P waves before QRS complexes in V5, V6 and lead II with short PR intervals. There is no definite AV dissociation, fusion or capture complexes.
According to Brugada's criteria, the WCT is more suggestive of ventricular tachycardia (VT) (Step 1: Absence of R wave in all precordial leads - No. Step 2: R to nadir of S >100 ms in 1 precordial lead - No. Step 3: AV dissociation - No. Step 4: Morphology criteria suggestive of typical LBBB - No (absence of notching in V6). The Brugada's criteria has a sensitivity of 98.7% and specificity of 96.5%. However, it misclassifies about 2% of WCT. It may not be able to differentiate SVT with conduction aberrancy from VT with septal origin. It does not differentiate pre-excited SVT / antidromic AV reentrant tachycardia from ventricular tachycardia.
According to the Verekei's criteria (modified aVR criteria), the WCT is more suggestive of VT (Step 1: Presence of initial R wave in aVR - Yes (small R wave in aVR - suggestive of VT); Step 2: Presence of initial Q wave or R wave duration in aVR >40ms - No; Step 3: Presence of notching on the descending limb of S wave and predominantly negative QRS in aVR - No; Step 4: Vi/Vt <=1 - Yes (Vi/Vt <1, suggestive of VT).
The aVR algorithm has greater sensitivity for VT diagnosis than the Brugada criteria
(96.5% vs 89.2%). The negative predictive values of aVR algorithms is higher than the Brugada algorithm (86.6% vs 67.2%). However, the algorithm may not be able to differentiate SVT with conduction aberrancy from VT of septal origin (e.g. fasicular VT, bundle branch reentrant VT, septal outflow tract VT). The algorithm does not differentiate SVT with conduction aberrancy from antidromic AVRT (e.g. atriofascicular accessory pathway/ Mahaim's fiber tachycardia).
According to Brugada's another algorithm (4) to differentiate antidromic AVRT from VT, the WCT is not suggestive of VT (Step 1: predominantly negative QRS in precordial leads in V4-6 - No. Step 2: Presence of QR complex in >=1 precordial leads from V2-V6) - No. Step 3: AV dissociation - No). However, the algorithm has only 75% sensitivity of diagnosing VT. Up to 25% of WCT meeting none of these criteria were actually VT.
By the WCT ECG morphology analysis, the LBBB morphology with superior axis and discordant QRS polarity in II/III and aVL/aVR is suggestive of right to left ventricular activation - due to either , SVT with LBBB, VT from lateral right ventricle, septal VT or antidromic AVRT associated with septal accessory pathway or right lateral accessory pathway. SVT with LBBB cannot have such supra-physiologically short PR duration during tachycardia. VT with 1:1 retrograde VA conduction or antidromic AVRT are still possible. Septal VT or septal accessary pathway is usually associated with earlier QRS transition (<= V3). The QRS transition is very late in V6 in this case, which is not typical of septal ventricular activation. Lateral right ventricular VT is usually associated with wider QRS duration due to slow activation via ventricular myocardium. The remaining likely diagnosis is antidromic AV reentrant tachycardia mediated by a right lateral accessory pathway inserting into the right bundle branch (atrio-fascicular AVRT/ Mahaim fiber tachycardia) (6). Mahaim fiber/atriofascicular accessory pathway is an antegrade conducting only accessory pathway connecting the atrium with the right bundle branch. Mahaim fiber tachycardia can mimic SVT with LBBB. The resting ECG may show minimal pre-excitation with LBBB-like morphology.
The use adenosine could help differentiate SVT from VT (as most VT could not be terminated by adenosine). Comparison with baseline ECG and invasive electrophysiology study could confirm the diagnosis. The most likely diagnosis in this case is antidromic AVRT mediated by an atriofascicular accessory pathway.
A is incorrect as the diagnosis of VT is not confirmed. Direct current cardioversion could not help differentiate VT from SVT or AVRT. The patient is hemodynamically stable. There is no need for cardioversion.
B is incorrect. Amiodarone as it could terminate both VT and SVT. It is long acting with long elimination half life. This will make electrophysiological diagnosis difficult as it suppresses both VT and SVT.
C is correct as adenosine could help differentiate VT from SVT (most VT could not be terminated by adenosine). It is short acting and does not interfere with electrophysiology study.
D is incorrect as the ST depression is due to repolarization change associated and not diagnostic of acute coronary syndrome in a 40year old lady without chest pain.
E is incorrect. Sodium bicarbonate should be given in case of suspected tricyclic anti-depressant (TCA) or flecainide poisoning. The clinical history does not suggestive the use of TCA or flecainide. The correct diagnosis is C.
