A 30-year-old woman presented to the clinic following a first episode of syncope. She had returned from the UK two days prior. Physical examination was unremarkable, and she denied any family history of cardiac disease.
What is the most appropriate next step in management?
Choose the correct answer.
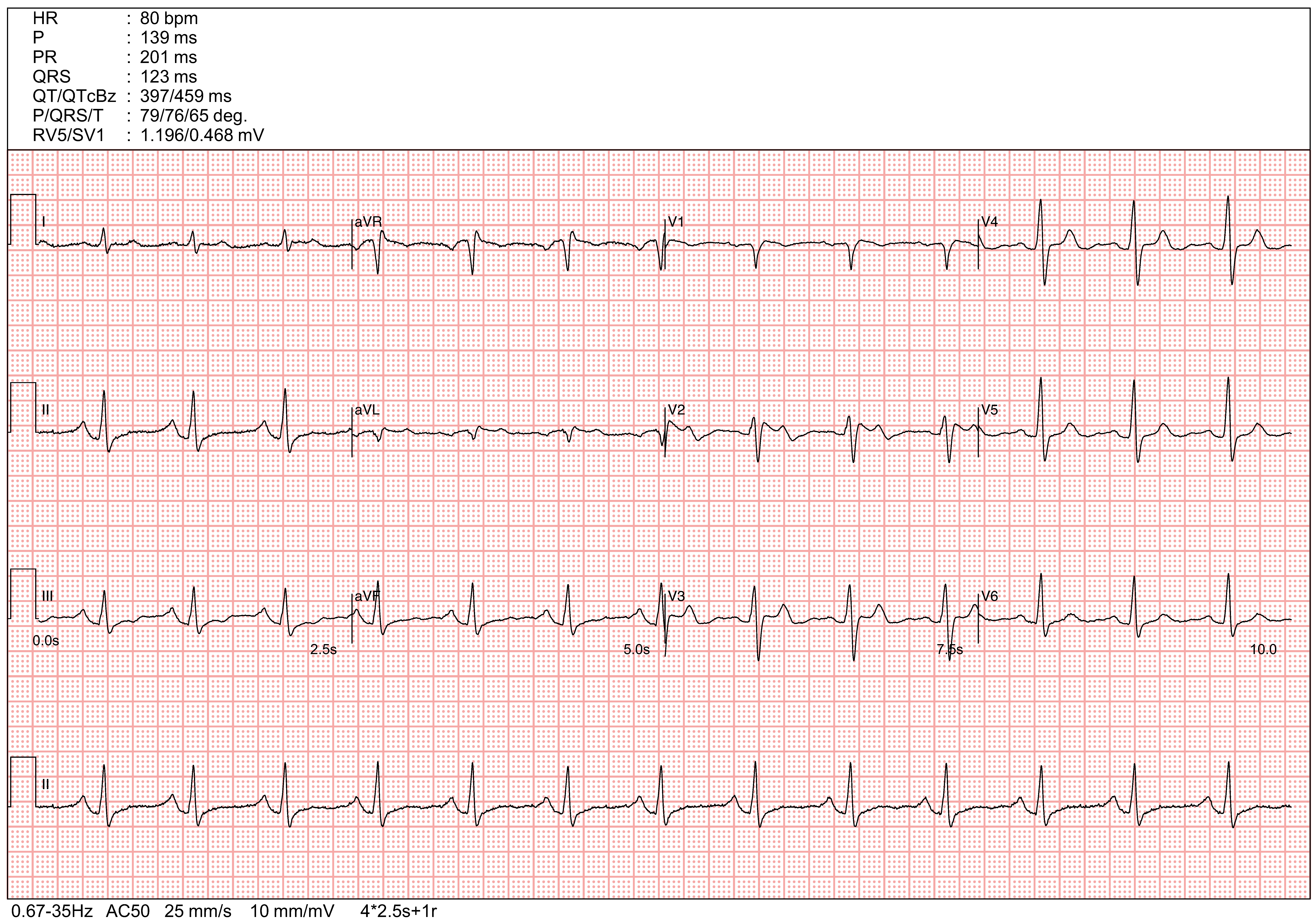
The index ECG demonstrates saddle-back ST-segment elevation (STE) in the right precordial leads (V1–V2), which is highly suggestive of a Type 2 Brugada pattern. While this pattern is not diagnostic of the syndrome on its own, it warrants further investigation. Sodium channel blockers, such as Flecainide or Ajmaline, can be used to unmask the condition by provoking a conversion into a diagnostic Type 1 Brugada pattern.
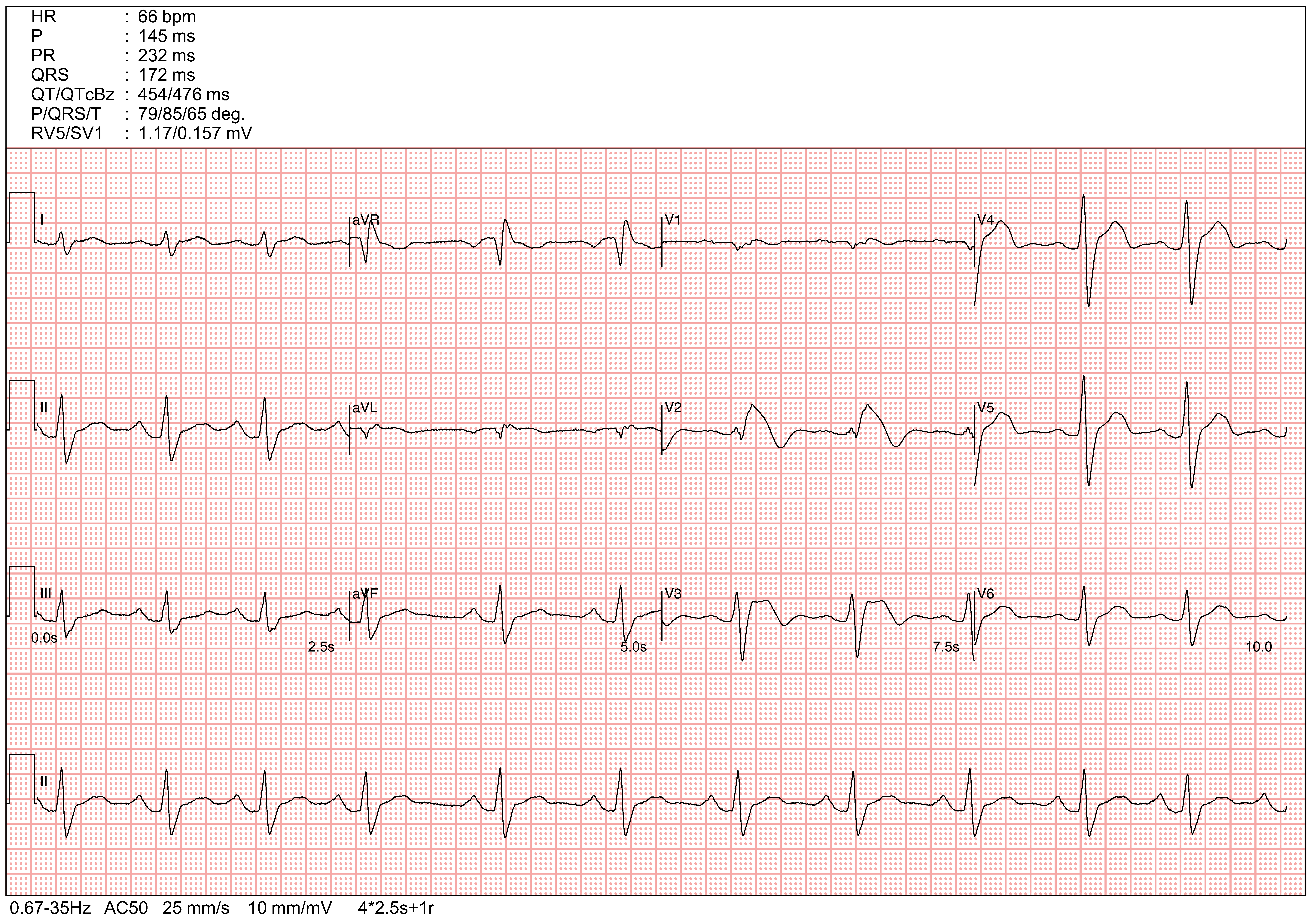
Following the administration of the Flecainide challenge test, the second ECG revealed Type 1 Brugada pattern, characterized by coved-type ST elevation ≥ 2 mm followed by a negative T-wave.
Brugada Syndrome is a genetic arrhythmia disorder that increases the risk of ventricular fibrillation and sudden cardiac death. Current clinical guidelines generally do not recommend ICD (Implantable Cardioverter-Defibrillator) implantation for patients who only exhibit a drug-induced Type 1 pattern for primary prevention without documented ventricular arrhythmia or aborted cardiac arrest. Conservative management and avoidance of triggering medications are typically preferred.
Further infomartion regarding Brugada Syndrome could be found in https://www.cardiologywiki.com/wiki/entities/brugada-syndrome/
It is critical to distinguish Brugada patterns from an Anterior STEMI. In the case of myocardial infarction, ST elevations are typically convex ("tombstoning") rather than saddle-back. Furthermore, the absence of reciprocal changes (ST depression in inferior leads) in this case suggests against a diagnosis of Anterior STEMI.
The most frequent ECG finding in pulmonary embolism is sinus tachycardia. While the classic S1Q3T3 pattern(deep S-wave in lead I, Q-wave and inverted T-wave in lead III) is a well-known sign of acute right heart strain, it is relatively infrequent and lacks sensitivity. Other findings reflecting right ventricular overload include a new right bundle branch block (RBBB) or T-wave inversions in leads V1–V3.
Acute pericarditis typically presents with diffuse ST-segment elevation across multiple leads, rather than being localized to the precordial leads. One key distinguishing feature of pericarditis is the presence of PR-segment depression(most notably in lead II) and PR-segment elevation in lead aVR.
