A 45-year-old lady presented to the AED with SOB and chest discomfort. She enjoyed good past health, including a normal CT coronary angiogram (CTCA) performed a few months ago.
Which of the following stagement is correct?
Choose the correct answer.
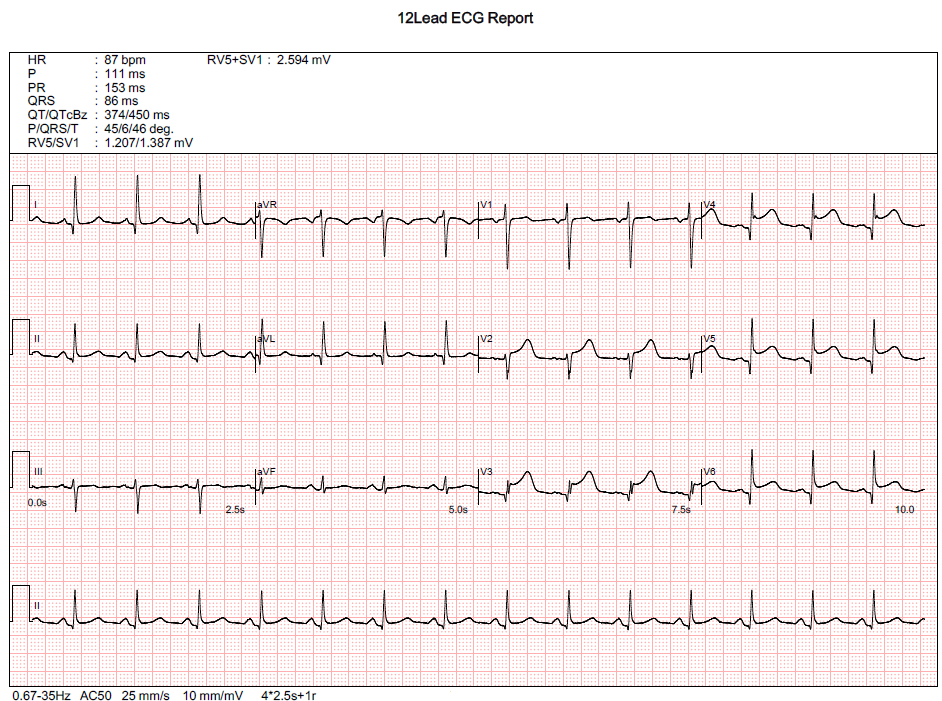
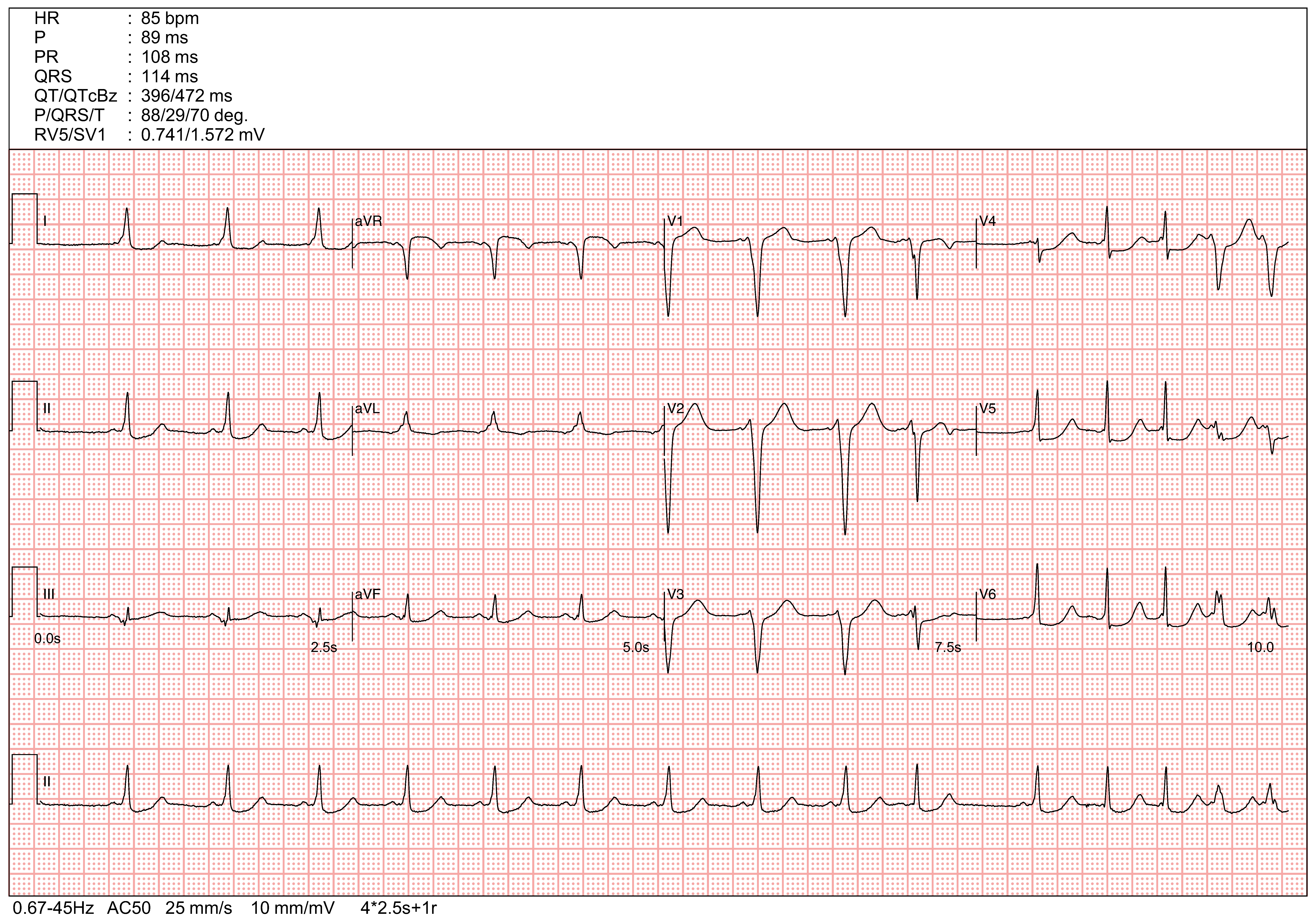
Index ECG showed ST segment elevation involving V2-6, compatible with Anterior STEMI. A recent normal CTCA cannot rule out non-plaque-related coronary obstructions, such as spontaneous coronary artery dissection (SCAD) or thrombotic occlusion.
However, the absence of reciprocal changes in Leads III and aVF, together with PR-segment depression in Leads II, V5, and V6, is not a typical finding of an anterior STEMI. Although anterior STEMI remains the provisional ECG diagnosis, alternative uncommon differentials should be considered, such as Takotsubo cardiomyopathy or concurrent peri-infarction pericarditis (PIP) masking reciprocal changes.
A bedside echocardiogram is highly valuable in this scenario. The absence of akinetic segments in the LAD distribution, together with apical ballooning and hypercontractile basal segments, is suggestive of Takotsubo cardiomyopathy.
However, a coronary angiogram remains mandatory, as Takotsubo cardiomyopathy is a diagnosis of exclusion.
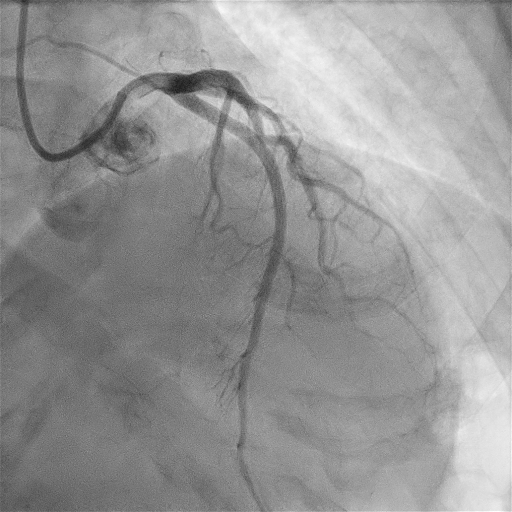
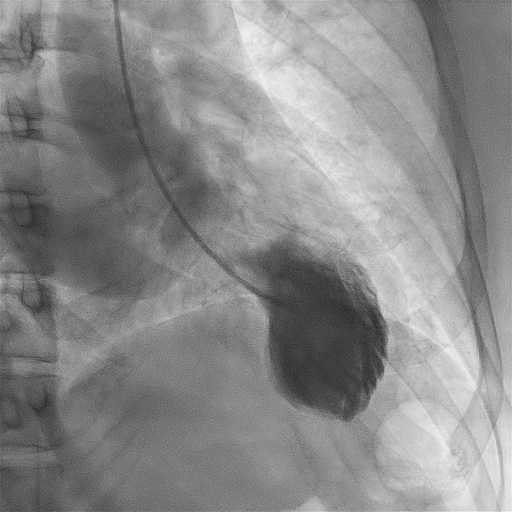
The coronary angiogram was normal. Left ventriculography (LV-gram) showed typical apical ballooning with preserved basal contractions. Cardiac MRI can provide markers for reversible injury (inflammation, ischemic edema) and irreversible damage (necrosis/fibrosis). This is particularly important for verifying the diagnosis of Takotsubo cardiomyopathy and excluding similar acute cardiac diseases, such as myocarditis.
The final diagnosis was Takotsubo cardiomyopathy.
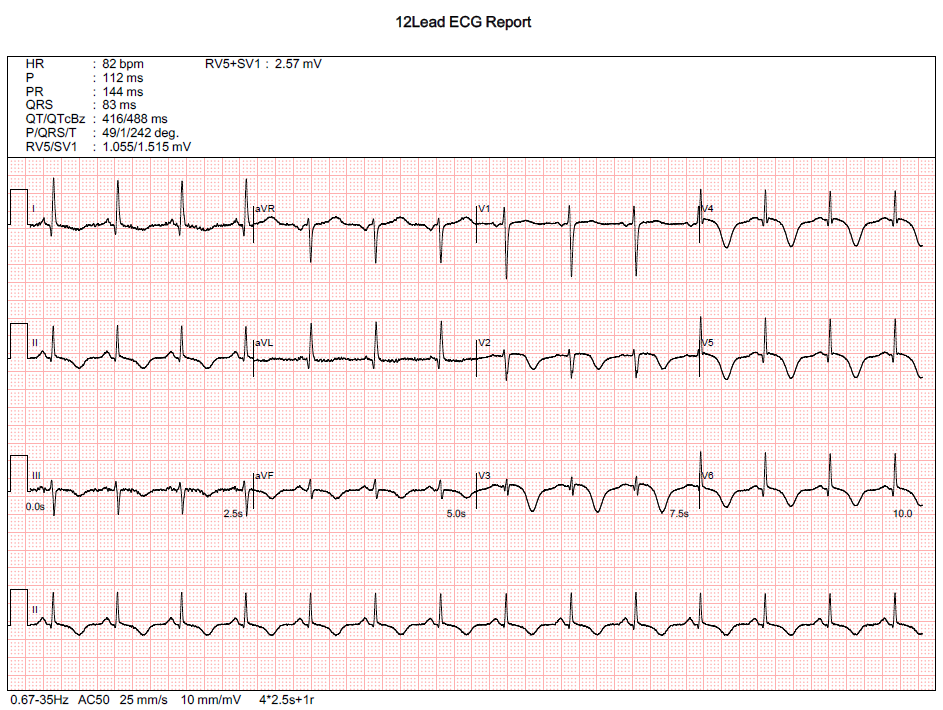
A follow-up ECG was performed a few days later, which showed resolution of the ST elevation along with new, diffuse T-wave inversions. This ECG finding suggests a global repolarization abnormality, commonly seen following diffuse myocardial injury.
Further information regarding Takotsubo cardiomyopathy cound be found in
The wide complex tachycardia (WCT) was terminated following treatment in the AED. A follow-up ECG was then performed.
Which of the following stagement is most approprite?
Choose the correct answer.
The follow up ECG shows sinus rhythm, with occasional atrial ectopics, short PR interval with delta waves.
The positive delta waves in V1 (with R<S in V1), I, II, aVF and negative delta waves in lead III are suggestive of right lateral accessory pathway.
The pre-excitation is incomplete due to fusion of electrical conduction between the AV node and the accessory pathway. In the last 2 QRS complexes, the QRS duration is widened with fully manifested pre-excitation following atrial ectopics. This is likely due to the electrical refractoriness of AV node following the atrial ectopics, allowing the electrical conduction predominantly going through the assessory pathway, which results in full pre-excitation.
The delta waves mophologies and QRS axis are similar with that in the WCT. The ECG finidngs in sinus rhythm further confirms the initial postulated diagnosis of anti-dromic AVRT mediated by a right lateral accessory pathway (most likely a atriofascicular accessory pathway/Mahaim fiber).
A is incorrect as the diagnosis is not suggestive of acute ST elevation myocardial infarction.
B is incorrect. The last 2 widen QRS complexes are likely due to atrial ectopics with fully manifested pre-excitation. The atrioventricular conduction predominatly goes through the accessory pathway rather than the AV node during the atrial ectopics when the AV node is made electrically refractory.
C is incorrect as amiodarone could block the accessory pathway and as long elimination half-life, which will make subsequent electrophysiology study/mapping and ablation of the pathway difficulty.
D is the correct answer. The patient has WPW and the previous wide complex tachycardia is likely an Antidromic Atrioventricular reentrant tachycardia (aAVRT).
E is incorrect as the diagnosis is suggestive of WPW with aAVRT.
