A 50-year-old man presented to the AED with acute chest pain, irregualr heart beats and dizziness today. His BP was 100/50 mmHg and SpO2 was 97% on room air.
Which of the following statement is correct?
Choose the correct answer.
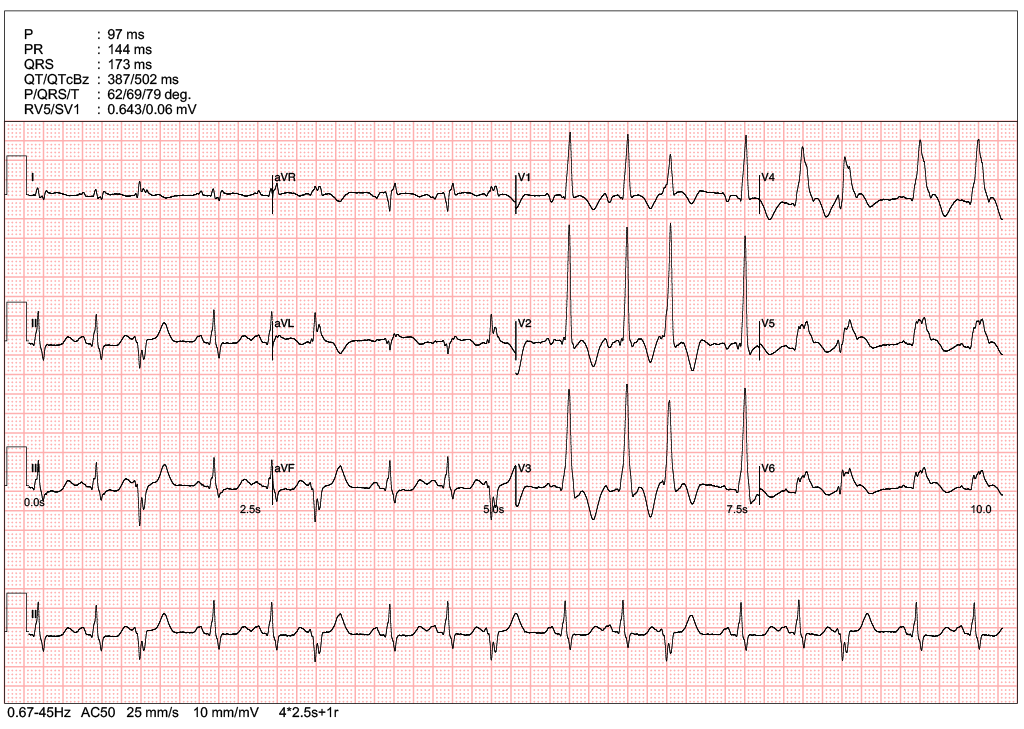
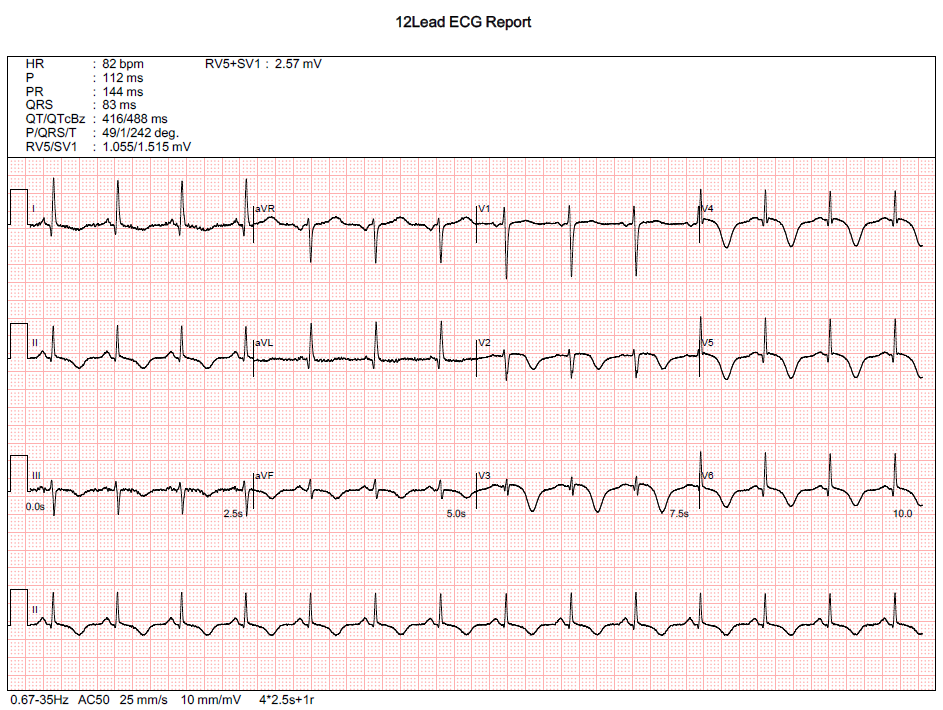
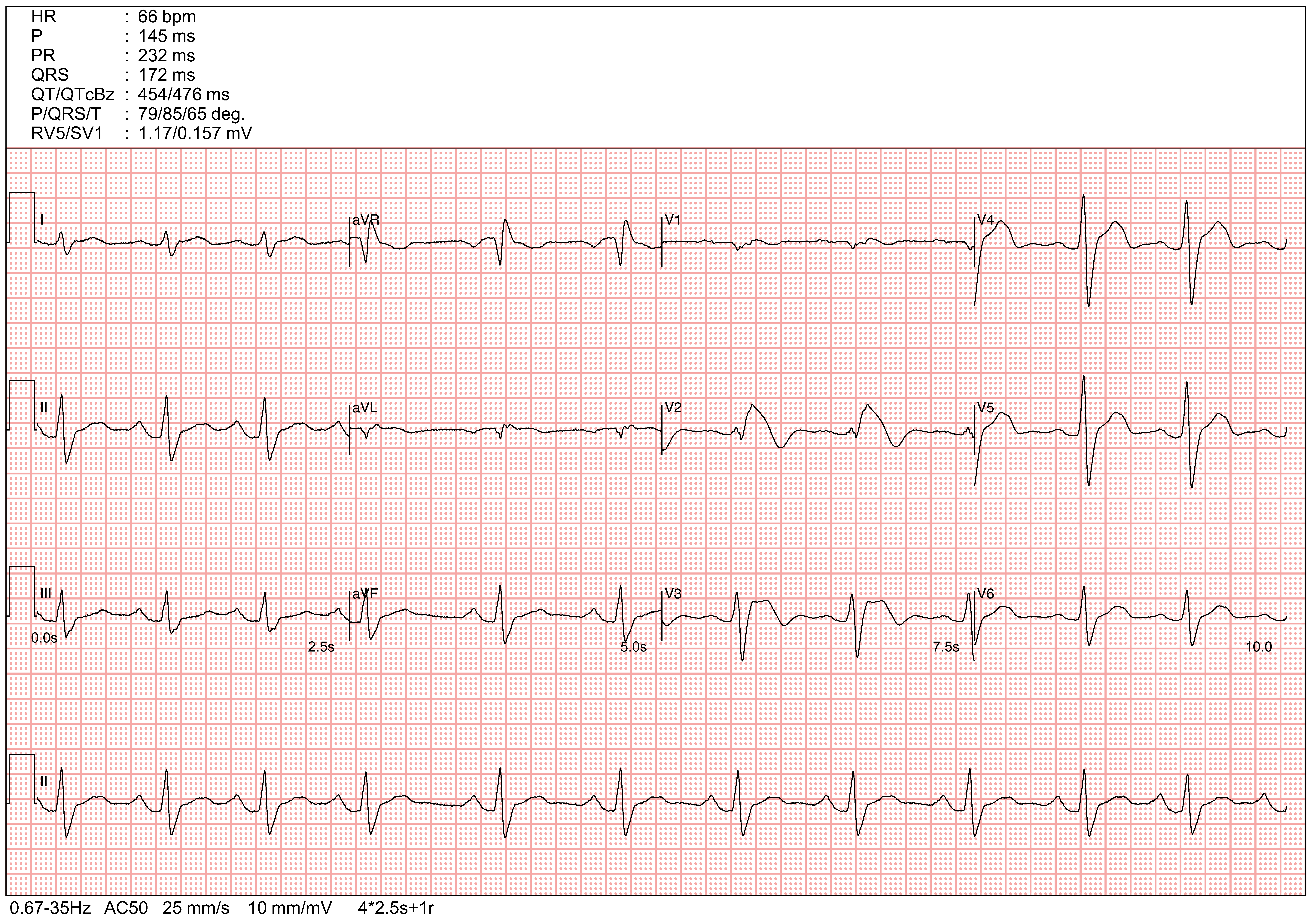
The presenting ECG shows ST-segment elevation in leads V4-V6, accompanied by reciprocal ST-segment depressions in the inferior leads (II, III, aVF) on natively conducted QRS complexes.
The presence of the reciprocal changes significantly enhances diagnostic specificity for a true STEMI, as the widening of QRS complexes in V4-V6 may otherwise mask the diagnosis of ST elevation
egarding the rhythm, clearly discernible P waves are present throughout the tracing, conclusively ruling out atrial fibrillation. Additionally, the documented QT interval prolongation should be recognized as a common secondary consequence of acute, ischemic myocardial injury rather than being assumed to indicate a primary drug-induced or congenital long QT syndrome. While taking a detailed medication history is a necessary component of the clinical workup for QRS widening, this investigative step must not delay immediate activation of primary PCI.
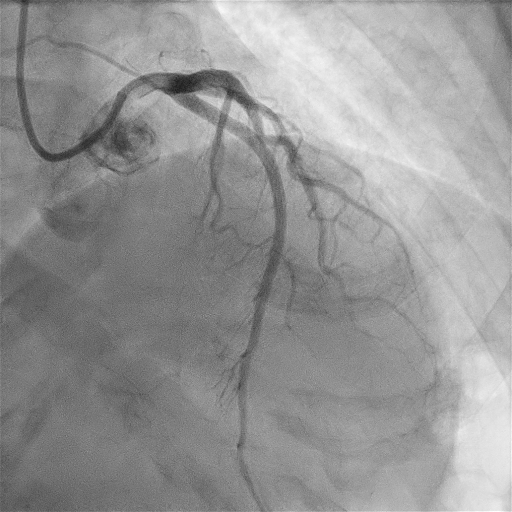
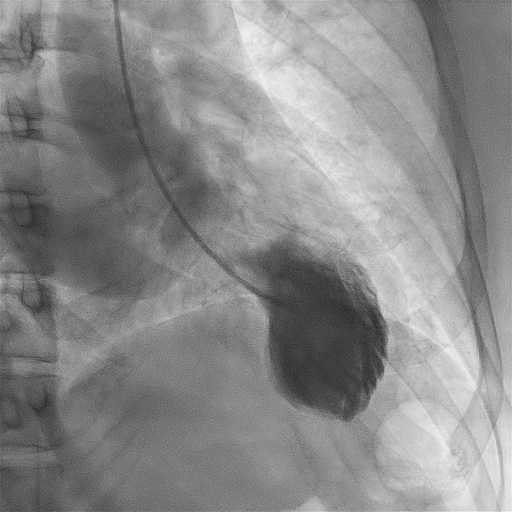
The coronary angiogram showed an acute total occlusion of the mid-LAD, which is consistent with apical transmural ischemia, especially in the context of a rotated heart.
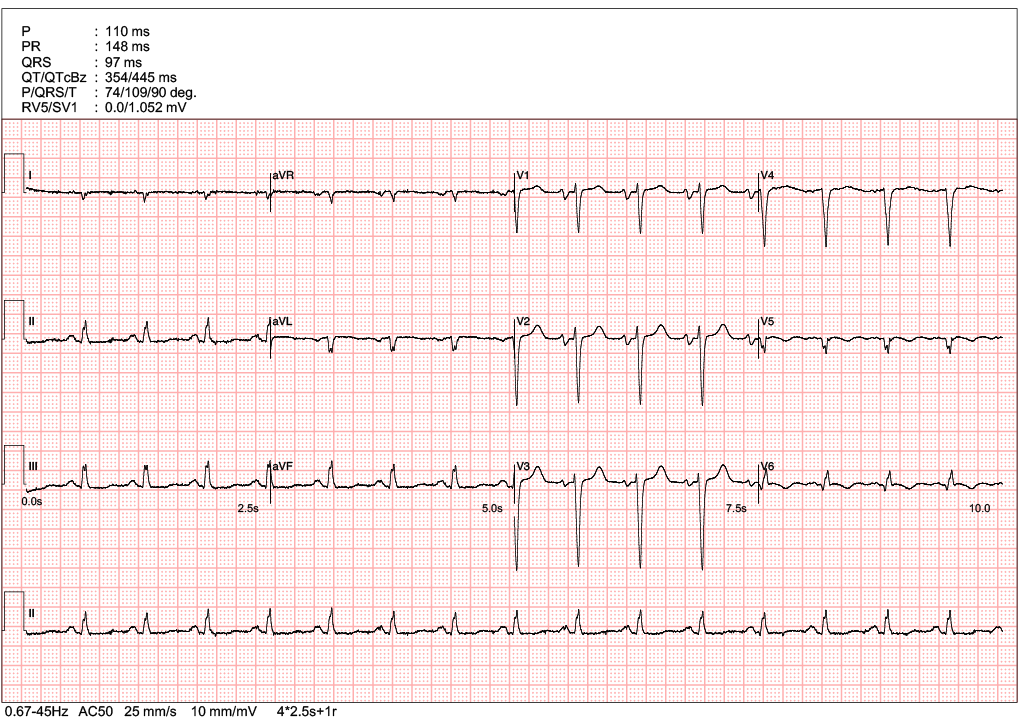
A post-PCI ECG is attached to evaluate for theexpected ST-segment resolution and confirm successful reperfusion.
A 45-year-old lady presented to the AED with SOB and chest discomfort. She enjoyed good past health, including a normal CT coronary angiogram (CTCA) performed a few months ago.
Which of the following stagement is correct?
Choose the correct answer.
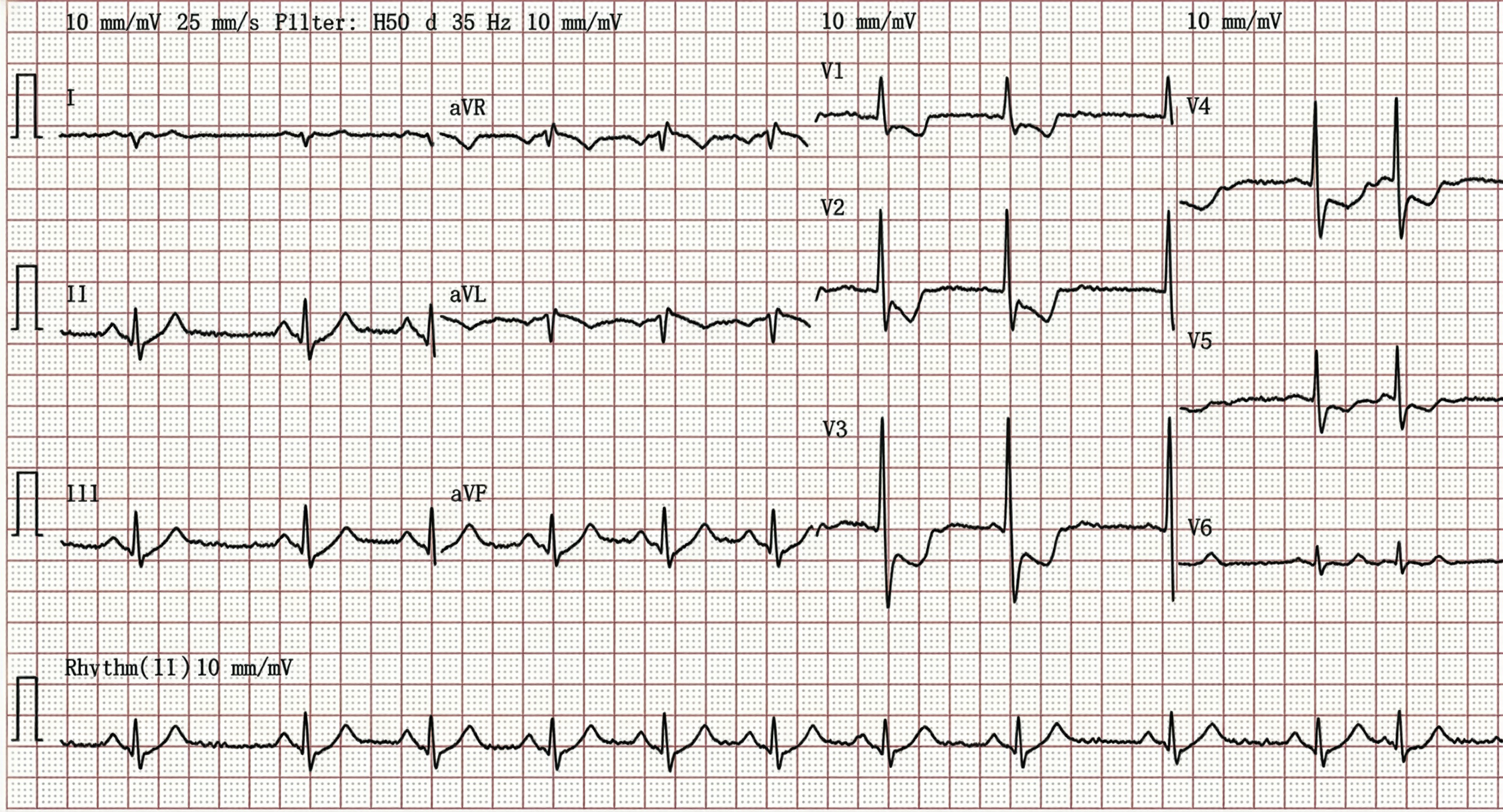
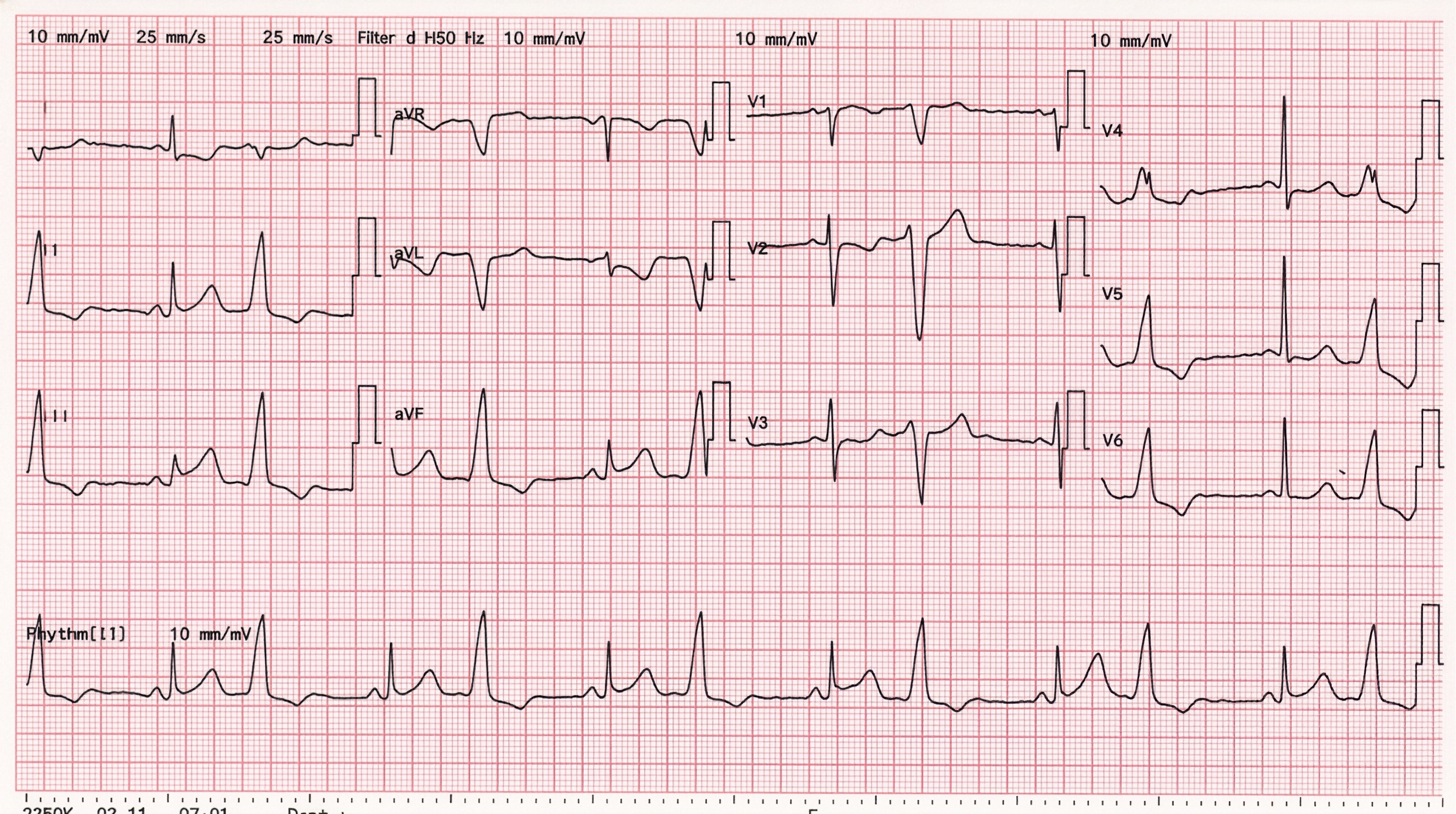
Index ECG showed ST segment elevation involving V2-6, compatible with Anterior STEMI. A recent normal CTCA cannot rule out non-plaque-related coronary obstructions, such as spontaneous coronary artery dissection (SCAD) or thrombotic occlusion.
However, the absence of reciprocal changes in Leads III and aVF, together with PR-segment depression in Leads II, V5, and V6, is not a typical finding of an anterior STEMI. Although anterior STEMI remains the provisional ECG diagnosis, alternative uncommon differentials should be considered, such as Takotsubo cardiomyopathy or concurrent peri-infarction pericarditis (PIP) masking reciprocal changes.
A bedside echocardiogram is highly valuable in this scenario. The absence of akinetic segments in the LAD distribution, together with apical ballooning and hypercontractile basal segments, is suggestive of Takotsubo cardiomyopathy.
However, a coronary angiogram remains mandatory, as Takotsubo cardiomyopathy is a diagnosis of exclusion.
The coronary angiogram was normal. Left ventriculography (LV-gram) showed typical apical ballooning with preserved basal contractions. Cardiac MRI can provide markers for reversible injury (inflammation, ischemic edema) and irreversible damage (necrosis/fibrosis). This is particularly important for verifying the diagnosis of Takotsubo cardiomyopathy and excluding similar acute cardiac diseases, such as myocarditis.
The final diagnosis was Takotsubo cardiomyopathy.
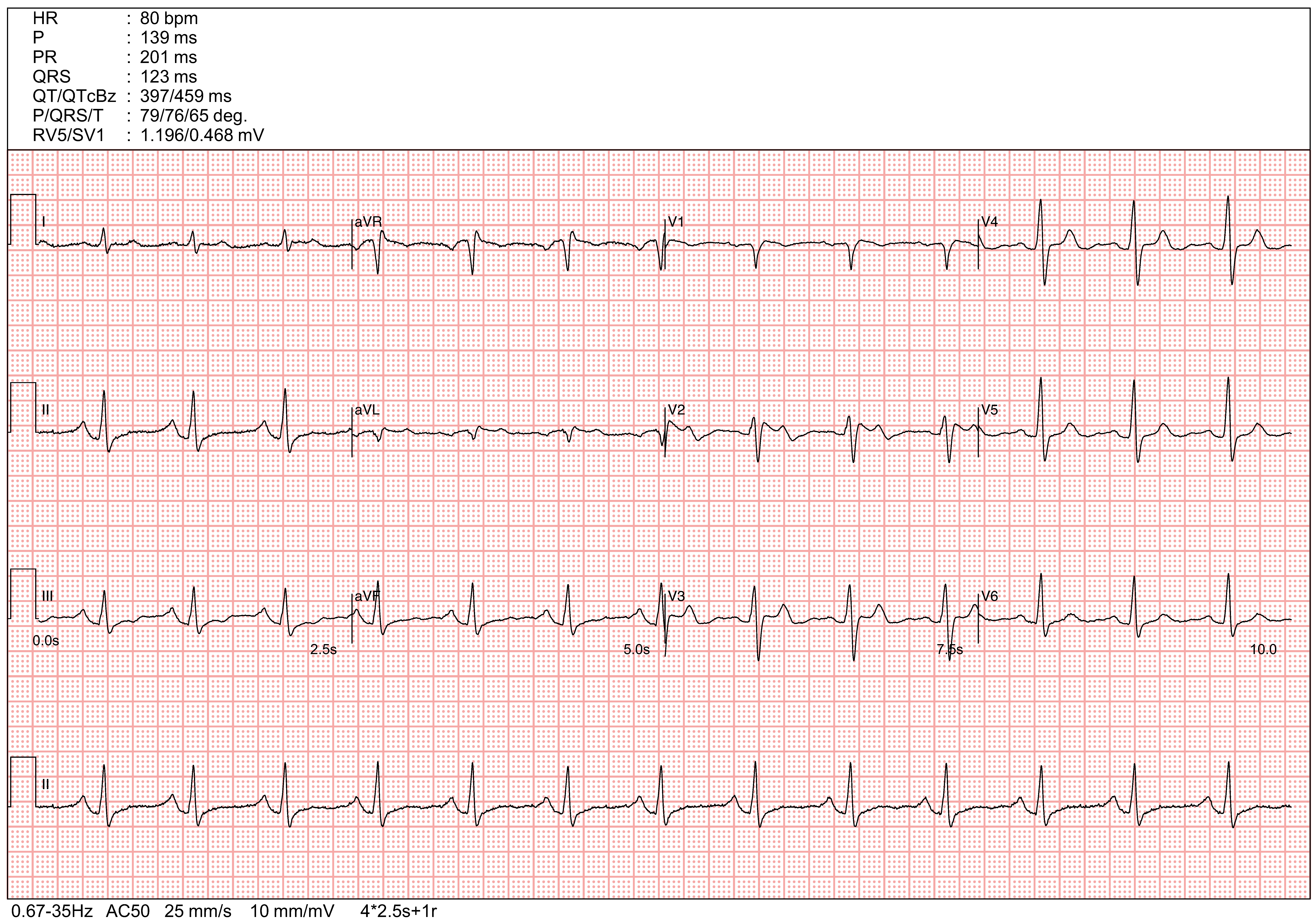
A follow-up ECG was performed a few days later, which showed resolution of the ST elevation along with new, diffuse T-wave inversions. This ECG finding suggests a global repolarization abnormality, commonly seen following diffuse myocardial injury.
Further information regarding Takotsubo cardiomyopathy cound be found in
A 70-year-old man presented to the AED with acute chest discomfort and SOB. His BP was 110/50 mmHg and SaO2 was 96% on 1L oxygen.
Which of the following is the most appropriate next step in management?
Choose the correct answer.
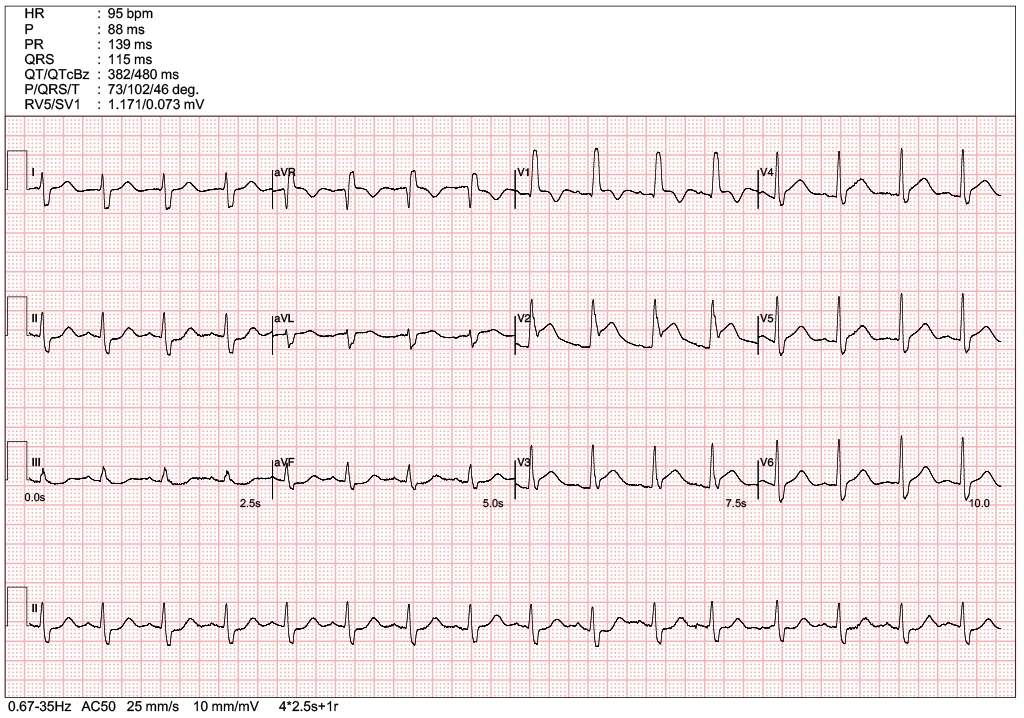
The ECG demonstrates ST-segment depression in leads V1–V3 with prominent R waves, a pattern highly suggestive of posterior STEMI. In such cases, the diagnosis could be further supported by evaluating the extended posterior leads V7–V9, which may reveal diagnostic ST elevation in some patients. Echocardiography provides crucial diagnostic verification when ECG findings remain equivocal. The most definitive finding is localized wall motion abnormality specifically involving the posterior segment of the left ventricle.
ST-T wave abnormalities associated with digoxin toxicity are usually diffuse and present across multiple leads, distinguishing them from the localized ischemic changes of a posterior infarction.
The most common ECG finding in pulmonary embolism (PE) is sinus tachycardia. In some patients, ECG findings may reflect acute right ventricular overload, manifesting as a new right bundle branch block (RBBB) or T-wave inversions in leads V1–V3, though significant ST-segment depression is less frequent. While the classic 'S1Q3T3' pattern (characterized by a deep S-wave in lead I, alongside a Q-wave and inverted T-wave in lead III) is suggestive of acute right heart strain, it is an infrequent finding with low sensitivity in clinical practice.
The presence of clearly identifiable P waves despite fluctuations in the atrial and ventricular rates is compatible with sinus arrhythmia rather than Atrial fibrillation.
A 30-year-old woman presented to the clinic following a first episode of syncope. She had returned from the UK two days prior. Physical examination was unremarkable, and she denied any family history of cardiac disease.
What is the most appropriate next step in management?
Choose the correct answer.
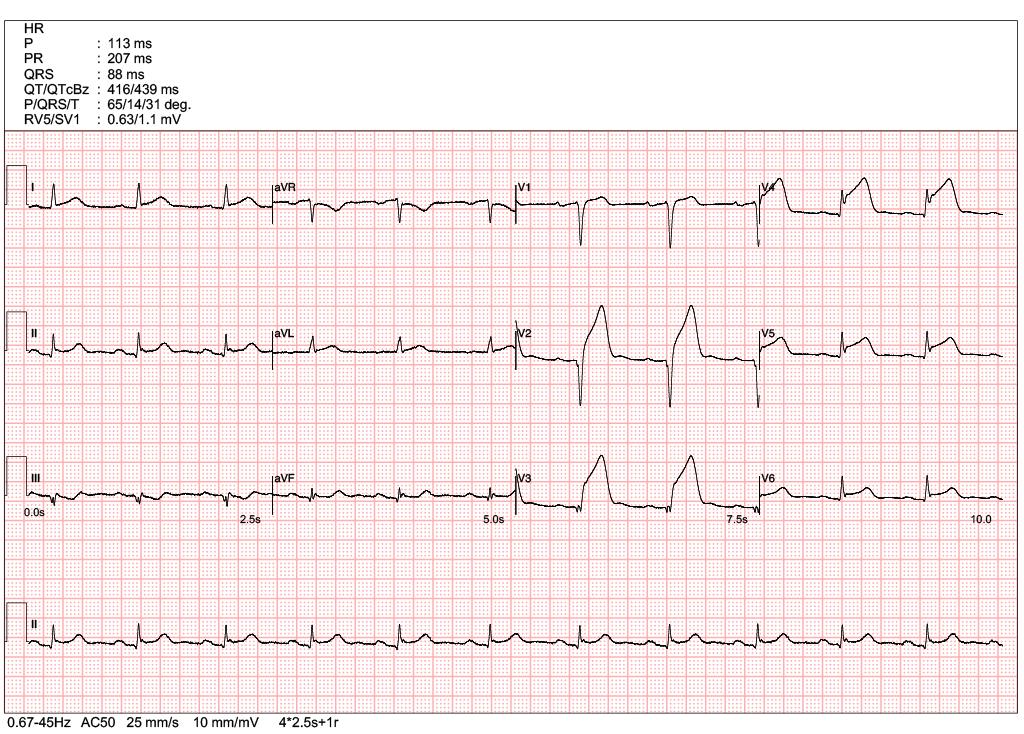
The index ECG demonstrates saddle-back ST-segment elevation (STE) in the right precordial leads (V1–V2), which is highly suggestive of a Type 2 Brugada pattern. While this pattern is not diagnostic of the syndrome on its own, it warrants further investigation. Sodium channel blockers, such as Flecainide or Ajmaline, can be used to unmask the condition by provoking a conversion into a diagnostic Type 1 Brugada pattern.
Following the administration of the Flecainide challenge test, the second ECG revealed Type 1 Brugada pattern, characterized by coved-type ST elevation ≥ 2 mm followed by a negative T-wave.
Brugada Syndrome is a genetic arrhythmia disorder that increases the risk of ventricular fibrillation and sudden cardiac death. Current clinical guidelines generally do not recommend ICD (Implantable Cardioverter-Defibrillator) implantation for patients who only exhibit a drug-induced Type 1 pattern for primary prevention without documented ventricular arrhythmia or aborted cardiac arrest. Conservative management and avoidance of triggering medications are typically preferred.
Further infomartion regarding Brugada Syndrome could be found in https://www.cardiologywiki.com/wiki/entities/brugada-syndrome/
It is critical to distinguish Brugada patterns from an Anterior STEMI. In the case of myocardial infarction, ST elevations are typically convex ("tombstoning") rather than saddle-back. Furthermore, the absence of reciprocal changes (ST depression in inferior leads) in this case suggests against a diagnosis of Anterior STEMI.
The most frequent ECG finding in pulmonary embolism is sinus tachycardia. While the classic S1Q3T3 pattern(deep S-wave in lead I, Q-wave and inverted T-wave in lead III) is a well-known sign of acute right heart strain, it is relatively infrequent and lacks sensitivity. Other findings reflecting right ventricular overload include a new right bundle branch block (RBBB) or T-wave inversions in leads V1–V3.
Acute pericarditis typically presents with diffuse ST-segment elevation across multiple leads, rather than being localized to the precordial leads. One key distinguishing feature of pericarditis is the presence of PR-segment depression(most notably in lead II) and PR-segment elevation in lead aVR.
A 50-year-old woman presented to the AED at 2:00 a.m. with palpitations and chest discomfort. Her BP was 90/50 mmHg and SaO2 99% on room air.
What is the most appropriate management?
Choose the correct answer.
The ECG demonstrates sinus rhythm with frequent PVCs in a bigeminal pattern, which may distract from the primary rhythm.
Notable ST elevation is present in the inferior leads of the conducted QRS complexes, with reciprocal changes in V2-V5, diagnostic of an inferior STEMI.
Given the morphology, the premature complexes are likely of RV outflow tract origin.
Management of an acute STEMI requires emergent reperfusion therapy; primary PCI is the preferred strategy, though fibrinolytic therapy should be administered if PPCI cannot be performed within 120 minutes of medical contact.
A 90-year-old man presented with acute chest discomfort and SOB. He is a heavy smoker with a history of recurrent admissions for COPD exacerbations. His BP was 120/80 mmHg and SpO2 was 88% on room air.
Which of the following is the most appropriate next step in management?
Choose the correct answer.
The ECG showed an RBBB with ST elevation in leads V1–V4, consistent with an anterior STEMI.
Patients with COPD and cor pulmonale—without acute myocardial infarction—should not exhibit ST elevation on the ECG. RV dilation in COPD patients can be attributed to cor pulmonale alone, even in the absence of a pulmonary embolism. A prolonged QTc without torsades de pointes does not warrant IV magnesium treatment
A 60-year-old man presented to the AED with intermittent chest pain of several days' duration. He could not recall the exact onset of the pain. His BP was 150/90 mmHg and SpO2 was 97% on room air.
Which of the following statement is correct?
Choose the correct answer.
The ECG showed ST-segment elevation in the Anterior leads (V2-4), consistent with an Anterior STEMI.
Although the exact onset time was unknown, it should not be treated as a delayed presentation because the chest pain was intermittent and persistent. Baseline ECG comparison is not mandatory for a diagnosis of STEMI, and overt reciprocal changes are not always present. Since obvious ST elevation was present on the initial ECG, serial ECGs are not necessary, thereby avoiding delay in revascularization
